
Does Coconut Oil Really Work for Alzheimer's?
The Mary Newport Coconut Oil Story (Part 1 of 3)

The Story That Started It All
If you’ve been researching natural approaches to Alzheimer’s disease, you’d likely have encountered Dr. Mary Newport’s remarkable story about coconut oil for dementia. Her husband, Steve Newport, was diagnosed with early-onset Alzheimer’s at age 51. Desperate to help him, Dr. Newport began giving him 4 tablespoons of coconut oil every day.
After just 60 days, signs of cognitive improvement began to show.
Steve could draw a clock face again (a standard cognitive test he’d previously failed).
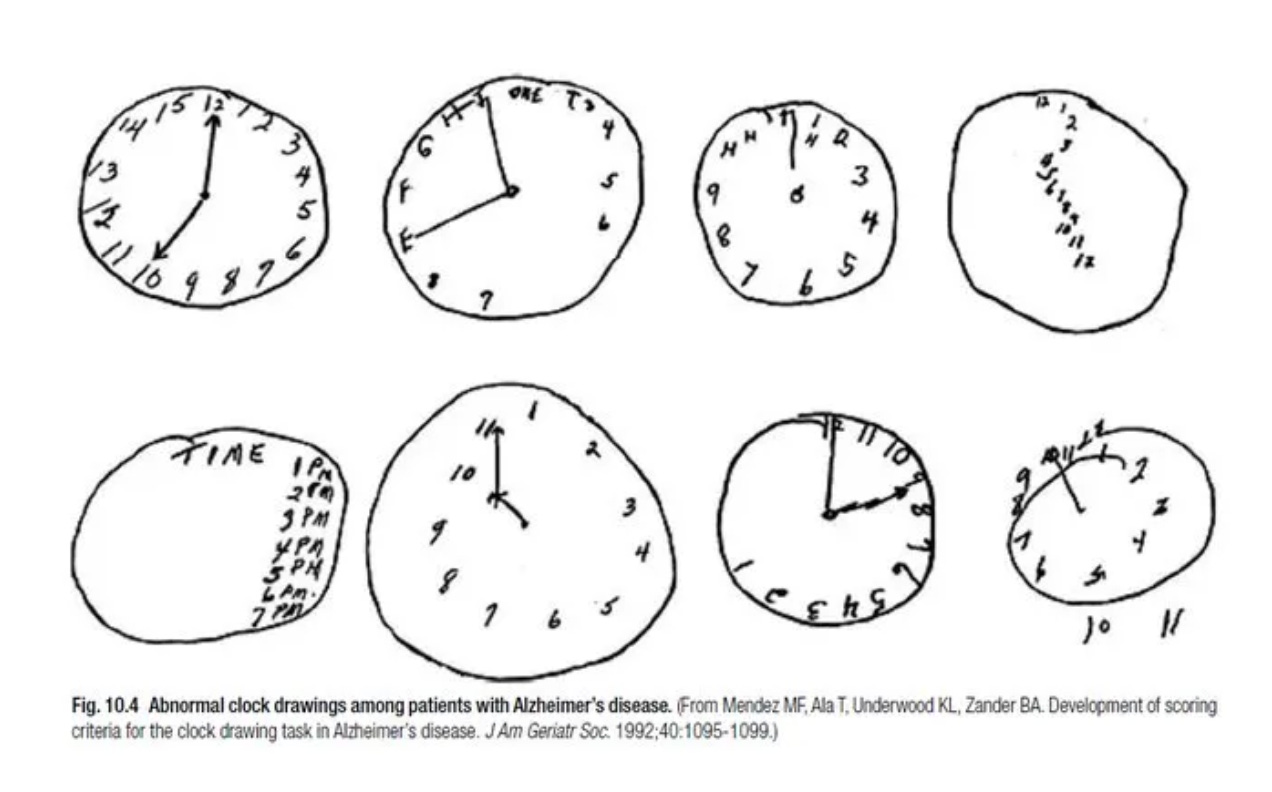
His tremors decreased. His mood brightened. He could remember events and hold conversations more clearly.
Since that breakthrough, Dr. Mary Newport has been advocating for the use of coconut oil — and MCT oil (which is also important) — in combating Alzheimer’s disease. Her story has inspired thousands of caregivers to try coconut oil for their loved ones with dementia.
But here’s the critical question: Is coconut oil for Alzheimer’s supported by science, or is it just one woman’s anecdotal success?
In this three-part series, we’ll examine:
Part 1 (this article): What Mary Newport discovered —> how coconut oil actually works in the brain.
Part 2: Why MCT oil might be superior to coconut oil, and the specific science behind different types of MCTs for brain health
Part 3: The complete picture —> all the oils that protect your brain, and evidence-based protocols for dementia prevention
Is coconut oil for Alzheimer’s supported by science, or is it just one woman’s anecdotal success?
What Makes Coconut Oil Different from Other Fats?

To understand why coconut oil for the brain might work, you need to understand how your brain gets energy.
Normally, your brain runs on glucose (sugar). But in Alzheimer’s disease, the brain loses its ability to use glucose effectively. Brain cells essentially starve —> they’re surrounded by fuel they can’t access.
This is where coconut oil becomes interesting.
The Medium-Chain Fatty Acid Advantage
Coconut oil is 90% saturated fat, but it’s not like the saturated fat in butter or beef. Over 50% of the fats in coconut oil are medium-chain fatty acids (MCFAs) — specifically chains of 8, 10, and 12 carbon atoms.
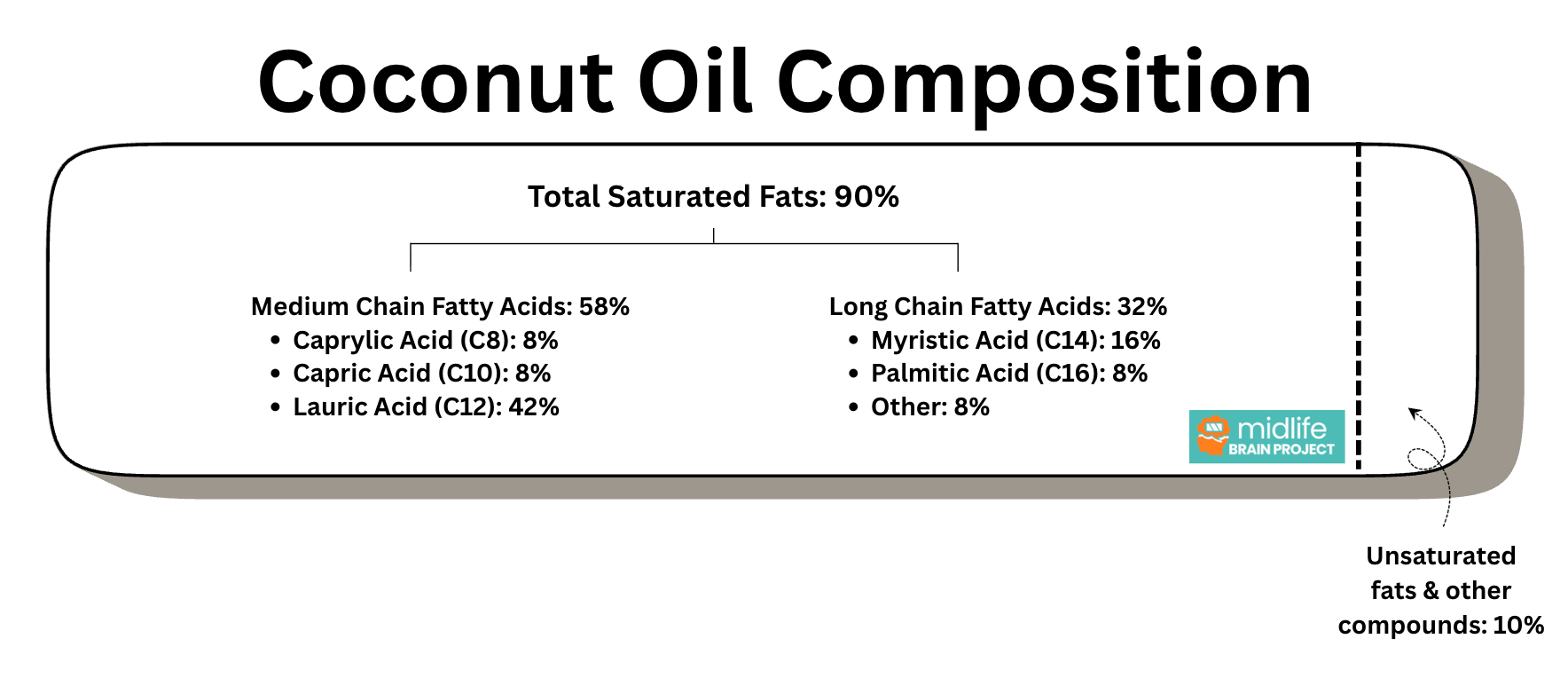
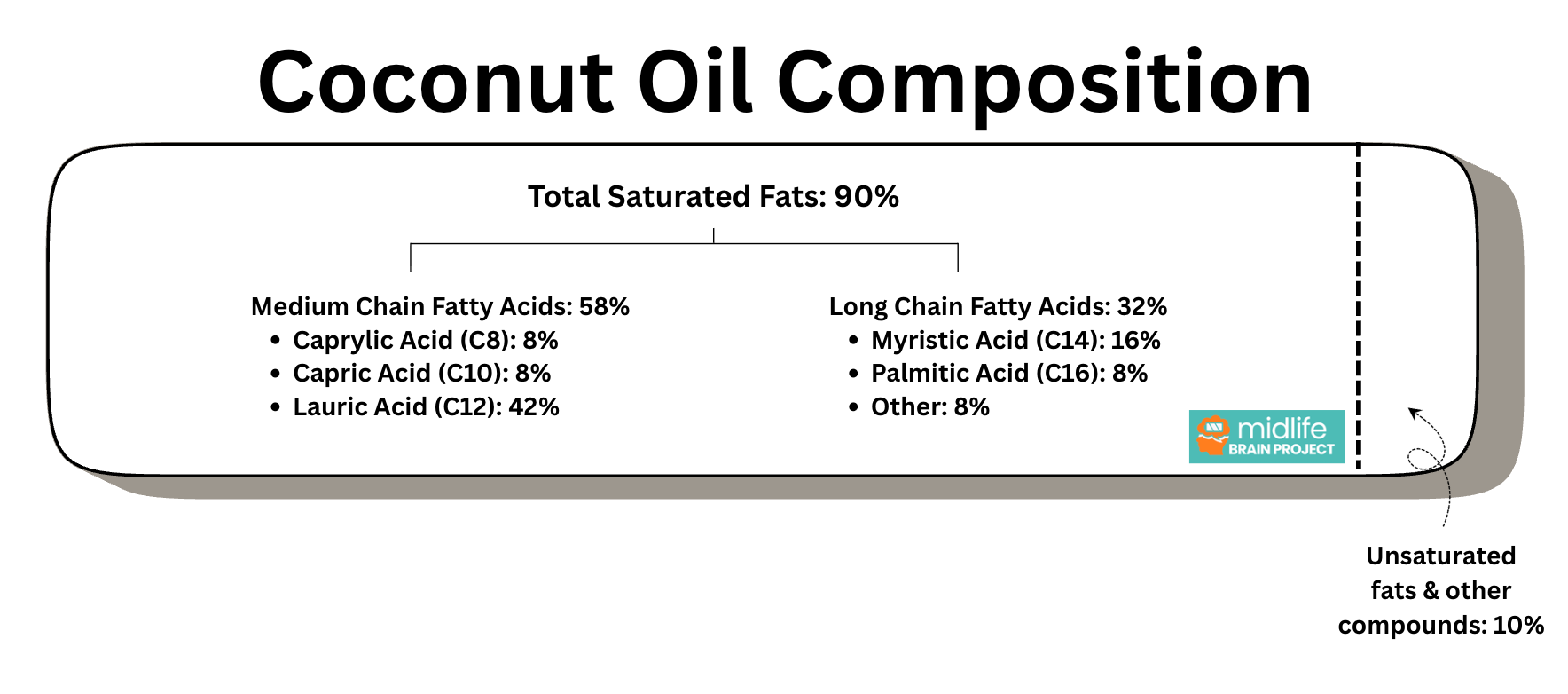
Here’s the complete breakdown of coconut oil composition:
Total Saturated Fats: 90%
Medium Chain Fatty Acids: 58%
Caprylic Acid (C8): 8%
Capric Acid (C10): 8%
Lauric Acid (C12): 42%
Long Chain Fatty Acids: 32%
Myristic Acid (C14): 16%
Palmitic Acid (C16): 8%
Other: 8%
Unsaturated Fats: 9% Other compounds: 1% (vitamin E, polyphenols)
Coconut oil is 90% saturated fat. Over 50% of the fats in coconut oil are medium-chain fatty acids (MCFAs). MCFAs are not long-chain, but they are still saturated fat.
How Your Body Processes These Fats Differently

Let’s dive deeper to understand how coconut oil works for the body, and more crucially, how it helps someone with dementia:
Long Chain Fatty Acids (LCFAs) from animal fats like butter and beef:
Require bile and pancreatic enzymes to digest
Get packaged into particles called chylomicrons
Travel through your lymphatic system
Eventually get stored as body fat if not needed immediately
Tend to stick to artery walls, contributing to atherosclerosis
Medium Chain Fatty Acids (MCFAs) from coconut oil:
Bypass normal digestion
Absorb directly through the small intestine
Go straight to your liver via the portal vein
Get rapidly converted into ketones
These ketones provide an alternative fuel source for your brain
MCTs from coconut oil —> ketones —> energy for the brain.
This is the key insight that Mary Newport discovered: When Steve’s brain couldn’t use glucose, the ketones from coconut oil gave his brain cells an alternative energy source they could use.
What Are Ketones and Why Do They Matter?

Ketones are small molecules your liver produces from fat. They’re like a backup generator for your brain.
Four reasons why Ketones are so special:
They easily cross the blood-brain barrier (BBB)
Brain cells can use them for energy without needing insulin
They’re the same fuel your brain uses during fasting and time restricted eating
They can “rescue” starving brain cells in Alzheimer’s disease
When you consume medium-chain fatty acids from coconut oil:
They reach your liver within minutes
Your liver converts them to ketones (primarily beta-hydroxybutyrate)
Ketones enter your bloodstream
They cross into your brain
Your brain cells use them as fuel
KEY DISTINCTION: This happens whether you’re on a ketogenic diet or not. The MCFAs in coconut oil produce ketones on their own.
When you directly consume MCFAs, your liver uses them to create ketones, and your brain uses them as fuel. You don’t have to be on a keto diet or fast for this to happen.
TLDR: The MCFAs in coconut oil bypass normal digestion and get converted directly to ketones, providing your brain with an alternative fuel source that works even when Alzheimer’s has damaged the brain’s ability to use glucose.
The Lauric Acid Paradox: Coconut Oil's Secret Weapon (and Problem)
Here’s where coconut oil gets complicated — something that most articles about coconut oil for Alzheimer’s get wrong.
Not All Medium-Chain Fatty Acids Are Created Equal
Look at that composition again. The single largest component of coconut oil is lauric acid at 42%.
Lauric acid has 12 carbon atoms. Technically, that makes it a “medium-chain” fatty acid. But here’s the catch: lauric acid acts biologically like a long-chain fatty acid.
Unlike the true MCFAs (C8 and C10) that go directly to your liver for ketone production, lauric acid:
Gets packaged into chylomicrons (like long-chain fats)
Takes the slow route through your lymphatic system
Raises LDL cholesterol (the “bad” cholesterol)
Behaves more like the saturated fat in butter than the ketone-producing C8 and C10
Think of lauric acid as an awkward middle child: too long to act like a true MCT, too short to be classified with the longer-chain fats.
Lauric acid is like the awkward middle child.
So Is Lauric Acid Good or Bad?
The answer: It’s “right of center”—bad for cardiovascular health, but not as bad as other saturated fats, and with some surprising redeeming qualities.
The cardiovascular concern:
Lauric acid raises LDL cholesterol like other long-chain saturated fats. This is a legitimate concern, especially for people already at cardiovascular risk.
The redeeming quality:
Lauric acid raises HDL cholesterol (the “good” cholesterol) even more than it raises LDL. Research shows that oils rich in lauric acid actually decrease the ratio of total cholesterol to HDL cholesterol.
A desirable ratio is 5:1, and an optimal ratio is 3.5:1
What really matters for cardiovascular risk isn’t just LDL by itself—it’s the ratio of total cholesterol to HDL. Lauric acid improves that ratio.
To put it simply: Lauric acid is bad because it raises LDL like other saturated fats, but it has redeeming qualities because it increases HDL in relation to total cholesterol. It’s not as harmful as palmitic acid from animal fats, but it’s not innocent either.
The Surprise: Lauric Acid is Actually Neuroprotective
Despite its cardiovascular concerns, lauric acid has remarkable effects on brain cells. This is the part that makes coconut oil for the brain more than just a ketone-delivery system.
Lauric acid is not just a source of ketones — it actually protects the brian!
Research shows that lauric acid:
Enhances growth factors (GDNF, IL6, CCL2) in astrocytes—the cells that nourish and support neurons
Increases presynaptic protein levels (supporting neuron-to-neuron communication)
Acts as a “lipid activator” for neuron-glial cell communication
Supports neuronal maturation and development
One study specifically tested lauric acid, capric acid (C10), and caprylic acid (C8) for their effects on brain cells. Lauric acid showed the strongest effects on neurotrophic factors—the growth factors that support and repair neurons.
Lauric Acid and Brain Inflammation

Here’s where it gets even more interesting. The standard argument against saturated fats is that they cause inflammation. And chronic neuroinflammation is a major driver of Alzheimer’s disease.
Lauric Acid is a “good” saturated fat — “good” in reducing brain inflammation!
But research specifically on lauric acid shows something different.
When tested in brain cells, lauric acid actually down-regulates:
Oxidative stress genes (GCLC, HO-1, Nqo1)
Inflammatory genes (IL6, TNFα, iNOS)
The research clearly shows that lauric acid inhibits neuroinflammation and provides cellular antioxidant activity that protects brain cells.
TLDR: Lauric acid (despite being a saturated fat) actually reduces brain inflammation rather than causing it. This makes it unique among saturated fats and explains why coconut oil might have special benefits for brain health beyond just ketone production.
Watch my video summary below👇👇 if you are too tired to read 😅
The Cardiovascular Truth No One Wants to Tell You

Ok, we’ve covered why MCFAs are good for your brain. We’ve given the pros and cons of letting lauric acid enter your system.
Now’s let’s be completely honest about what happens when you follow Mary Newport’s coconut oil protocol for Alzheimer’s.
What’s Actually Problematic in Coconut Oil?
Remember that composition? Let’s categorize it by cardiovascular impact:
Fats that act like long-chain fatty acids (problematic for cardiovascular health):
Lauric Acid (C12): 42%
Myristic Acid (C14): 16%
Palmitic Acid (C16): 8%
Other LCFAs: 8%
Total: 74% of coconut oil acts like long-chain saturated fat in your cardiovascular system
Only the C8 (8%) and C10 (8%)—totaling just 16%—are the “clean” MCFAs that produce ketones without cardiovascular concerns.
Dr. Mary Newport’s Actual Dosage Recommendation
In her book and talks, Dr. Mary Newport recommends 3-6 tablespoons of coconut oil daily for Alzheimer’s prevention or treatment.
Let’s calculate what 6 tablespoons actually means for your cardiovascular system:
6 tablespoons = approximately 84g of total fat
90% is saturated fat = 75.6g saturated fat
74% acts like LCFA = approximately 56g of LDL-raising saturated fat
The American Heart Association recommends: 11-13g saturated fat per day
Despite the latest change in the food pyramid, the American Heart Association (AHA) still recommends aiming for less than 6% of total daily calories from saturated fat, a stricter guideline than the general U.S. Dietary Guideline of under 10%; this translates to about 13 grams or less on a 2,000-calorie diet, emphasizing whole foods, plant-based proteins, and healthy fats like olive oil to reduce artery-clogging cholesterol.
Mary Newport’s protocol is 2.5-3 times the recommended daily limit of saturated fat— not just slightly over, but several times higher.
(NOTE: there is a strong caveat here from other substack writers who write about how saturated fats are not as harmful as the AHA says, but my writing is just based on what I know as of now.)
That’s 350-700 calories from coconut oil alone, before you’ve eaten any actual food.
Does Coconut Oil Actually Raise Cholesterol?
Yes. Harvard University research conducted a meta-analysis of 16 clinical trials examining coconut oil consumption:
Results:
Total cholesterol increased by about 15 points
LDL (”bad” cholesterol) increased by 10 points
HDL (”good” cholesterol) increased by 4 points
The HDL increase from coconut oil may be insufficient to effectively “cancel out” the LDL increase. While the total:HDL ratio improves, the absolute increase in LDL is still concerning for many people.
The Real Risk-Benefit Calculation
Here’s what this means in practical terms:
If you want your brain to be healthier with coconut oil, be prepared to pay a cardiovascular price.
You can mitigate this risk with:
Regular vigorous exercise is absolutely essential ← this is non-negotiable
Avoiding smoking (obviously)
Managing stress
Reducing carbohydrate intake (to support ketone production)
Monitoring your lipid panel every 3 months initially
But even with all of this, you’re still consuming 2.5-3× the recommended saturated fat intake.
For some people — especially those with excellent cardiovascular health, regular exercise habits, and no genetic predisposition to high cholesterol — this may be an acceptable trade-off if they or a loved one has Alzheimer’s disease.
For others — especially those with existing cardiovascular disease, high baseline cholesterol, or strong family history of heart disease — this could tip the scales toward a heart attack or stroke.
What Mary Newport Doesn’t Tell You
To be fair to Dr. Newport, she acknowledges in comments and talks that:
Not everyone responds the same way
Cardiovascular health must be monitored
Diet and exercise are important alongside coconut oil
Some people may need to adjust dosage based on their response
However, her primary focus remains on the cognitive benefits she saw in her husband. The cardiovascular risks are mentioned but not emphasized proportionally to their significance.
We also don’t know:
Steve Newport’s complete cardiovascular health outcomes long-term
His genetic risk factors (like APOE4 status)
His baseline lipid levels or how they changed
Whether he had any cardiovascular events
The focus is rightly on his cognitive improvements—but that’s only half the health equation.
So... Does Coconut Oil for Alzheimer’s Actually Work?

Based on the evidence, here’s the honest answer:
Yes, coconut oil can provide real benefits for brain health through:
Ketone production from C8 and C10 MCFAs (16% of coconut oil)
Neuronal support and anti-inflammatory effects from lauric acid (42% of coconut oil)
Alternative brain fuel when glucose metabolism is impaired
But it comes with a significant cardiovascular price:
74% of coconut oil raises LDL cholesterol like long-chain saturated fat
Mary Newport’s recommended dose (6 tablespoons) provides 2.5-3× the daily saturated fat limit
This requires excellent baseline cardiovascular health and regular monitoring
The risk-benefit calculation depends on your situation:
For someone with early Alzheimer’s or MCI: The potential cognitive benefits may outweigh cardiovascular risks, especially if:
Quality of life is already significantly impaired
Conventional treatments have limited effectiveness
Cardiovascular health is monitored closely
Exercise and diet are optimized
For someone in their 40s-50s trying to prevent dementia: The cardiovascular risks may outweigh the benefits, especially since:
Prevention is about long-term health across all systems
Heart disease is itself a major dementia risk factor
There may be better approaches with similar brain benefits but no cardiovascular downside
Key Takeaways from Part 1
Coconut oil for Alzheimer’s is based on real science (ketone production, alternative brain fuel)
Only 16% of coconut oil (the C8 and C10) produces ketones without cardiovascular concerns; 74% acts like long-chain saturated fat that raises LDL cholesterol
Lauric acid (42% of coconut oil) is paradoxical: It raises LDL but also raises HDL more, and it has unique neuroprotective and anti-inflammatory properties for brain cells
Mary Newport’s protocol (6 tablespoons daily) provides 2.5-3× the recommended saturated fat intake ← this is not a minor increase
Coconut oil may work for the brain but at a cardiovascular price that requires careful monitoring and may not be appropriate for everyone
The real question is: Can we get the benefits without the risks by using more targeted approaches?
The Critical Question
What if we could get the brain benefits of coconut oil without the cardiovascular risks?
What if we could:
Get pure, concentrated MCFAs (C8 and C10) without the problematic long-chain fats?
Understand exactly which component does what, so we can optimize our approach?
Combine the best aspects of different oils to create a more complete brain protection protocol?
This is exactly what we’ll explore in Part 2: MCT Oil vs. Coconut Oil — Why MCT Might Be Superior for Your Brain.
In that article, we’ll examine:
How MCT oil is made and what makes it different from coconut oil
How C8 (caprylic acid) produces 3-6× more ketones than lauric acid
The surprising differences between C8, C10, and C12 for brain metabolism
Why Dr. Newport ended up recommending a combination of MCT oil and coconut oil (not just coconut oil alone)
Practical protocols for different goals (prevention vs. treatment)
In the next article, we’ll explore why many researchers and clinicians have moved from coconut oil to MCT oil for cognitive support, what the science shows about different MCT formulations, and why even Dr. Mary Newport ended up recommending a combination approach rather than coconut oil alone.
This article is for educational purposes only and is not medical advice. Consult with a qualified healthcare provider before starting coconut oil, MCT oil, or any supplement protocol, especially if you have existing health conditions or take medications.
Helpful post! “Coconut oil for Alzheimer’s” sits right at the intersection of a real physiologic idea and a lot of overreach. The kernel of plausibility is metabolic: in some patients with AD or MCI there’s reduced cerebral glucose utilization, and ketones can serve as an alternative fuel. But coconut oil is a very blunt tool for that, its fatty acid profile is mostly saturated fat, and while it contains some MCTs, it’s not the same as a standardized MCT formulation used in trials. So the evidence for meaningful cognitive benefit is limited and inconsistent, and any potential upside needs to be weighed against cardiometabolic risk in the individual (LDL/apoB response can be substantial in some people). What I’d add for our longevity-focused readers is a practical, safety-first approach:
1. If someone wants to experiment, do it as a time-limited, trackable trial (sleep, function, cognition/behavior notes), and don’t let it displace the interventions with stronger evidence: vascular risk control, hearing/sleep optimization, exercise, and appropriate meds.
2. If there’s known dyslipidemia or high ASCVD risk, be cautious; consider MCT oil (in small doses) rather than large amounts of coconut oil, and monitor lipids.
3. And if symptoms are changing, prioritize a proper cognitive workup rather than chasing a single “superfood” answer.
Great write up and looking forward to the MCT article.
I know you didn't say "LDL should be as low as possible" but there are other benefits to LDL. Do you believe that we should be keeping cholesterol with the current guidelines? Or do you think that only applies when APO, immune impairment, or high iron suggest a risk of arterial plaques? Maybe another article idea for you.